The “is silicone safe” question lands in our inbox more than any other. The short answer customers want and the precise answer the compliance file actually supports are not always the same. Both deserve to be on the same page.
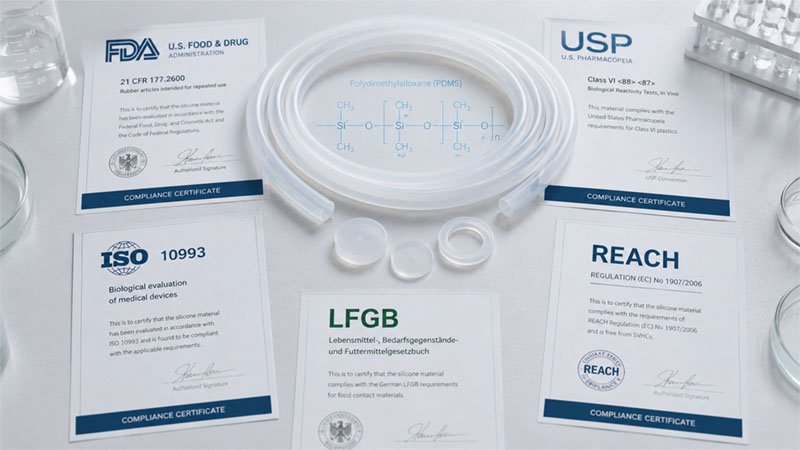
Pure platinum-cured silicone certified to FDA 21 CFR 177.2600, LFGB §30/§31, USP Class VI, and ISO 10993 is chemically inert, non-toxic, hypoallergenic, and approved for food contact, skin contact, mouth contact, and short-term implantation. The “safe” label depends on cure system, residue control, pigment compliance, and the specific regulation invoked — not on the word “silicone” alone.
This is the toxicology-and-compliance reference we hand to brand teams, parents, medical-device buyers, and regulatory reviewers before they decide whether a silicone product fits a specific use case.
What “Silicone” Actually Is
A lot of safety confusion starts at the chemistry.
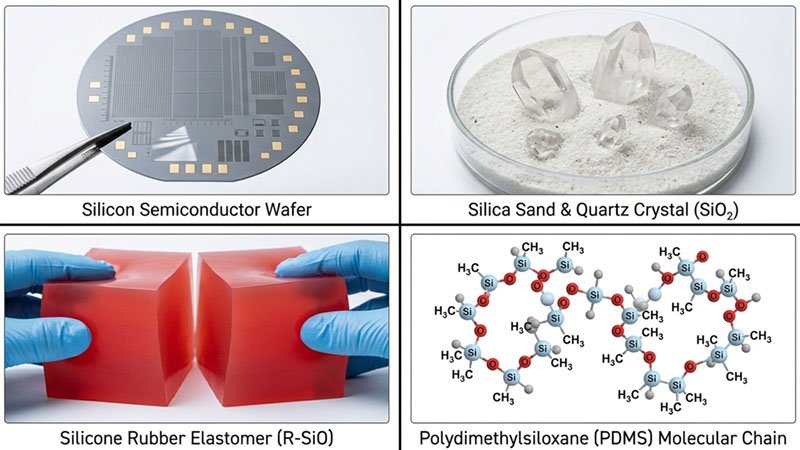
- Silicon (no “e”) is element 14 on the periodic table — a gray metalloid mined from quartz.
- Silica is silicon dioxide (SiO₂) — sand, glass, quartz.
- Silicone is a synthetic polymer with a backbone of alternating silicon and oxygen atoms (Si-O-Si), with organic side groups (typically methyl). The most common grade is polydimethylsiloxane, PDMS.
- Siloxanes are the building blocks of silicone — short-chain Si-O molecules. Specific cyclic siloxanes (D4, D5, D6) are regulated; the cured polymer made from them is not.
For the distinction in detail, see Silicon VS Silicone. The toxicology profile in this article applies to cured polymeric silicone (PDMS) — not to silica, not to silanes, not to silicone caulks or sealants with solvent carriers.
Five Compliance Standards That Define “Safe”
“Silicone is safe” is not a chemistry statement on its own. It is a compliance claim against one or more of the following standards.
| Standard | Jurisdiction / Use | What It Tests | Pass Criterion |
|---|---|---|---|
| FDA 21 CFR 177.2600 | US — food contact | Extractables into water (7-hr reflux) and n-hexane | ≤ 20 mg/in² water-extract; ≤ 175 mg/in² total |
| LFGB §30/§31 (BfR Rec. XV) | EU — food contact | Sensory + simulant migration + heavy-metal screen | No taste, odor, or color transfer; specific migration limits |
| USP Class VI | US — pharma / medical | Systemic, intracutaneous, and intramuscular toxicity in animal models | No biological reactivity at 50 / 70 / 121 °C extraction |
| ISO 10993-5/10/23 | Global — medical devices | Cytotoxicity, sensitization, irritation (skin / mucosa / implant) | Test panel dictated by contact type and duration |
| California Prop 65 | US-CA — consumer disclosure | Listed carcinogens, reproductive toxicants, heavy metals | Warning required above safe-harbor levels |
A product certified to one standard is not automatically certified to another. FDA food-contact approval does not cover medical use; USP Class VI does not cover food contact. A medical-grade silicone may still need a separate LFGB Declaration to be sold as European bakeware. For the why, see Food-Grade vs Medical-Grade Silicone.
Is Silicone Toxic?

No — pure cured silicone is not toxic by any of the routes that matter for product safety: oral, dermal, inhalation, or systemic.
The reasons are structural:
- Inert backbone. Si-O-Si is one of the most stable bonds in organic chemistry. It does not react with stomach acid, saliva, skin oils, blood, or household cleaners under normal conditions.
- No measurable leaching. Properly cured food-grade silicone shows extractables an order of magnitude below FDA limits. See Silicone Sheets Material Migration and Leaching Tests for an example data set.
- No BPA, no phthalates, no halogens. These plasticizers and stabilizers used in PVC and some polycarbonates are not part of the silicone formulation. For the comparison, see PVC vs Silicone and Silicone VS Plastic.
- Low surface energy. Silicone resists bacterial adhesion better than most polymers, which is why it dominates medical tubing and baby feeding products.
The full discussion is in Are Silicone Toxic?. The headline holds: pure platinum-cured silicone is non-toxic. The exceptions in the next sections are all about how a part is made or what is added to it — not about silicone itself.
What About D4, D5, D6 Cyclic Siloxanes?
This is the question regulatory reviewers ask first, and it deserves a precise answer.
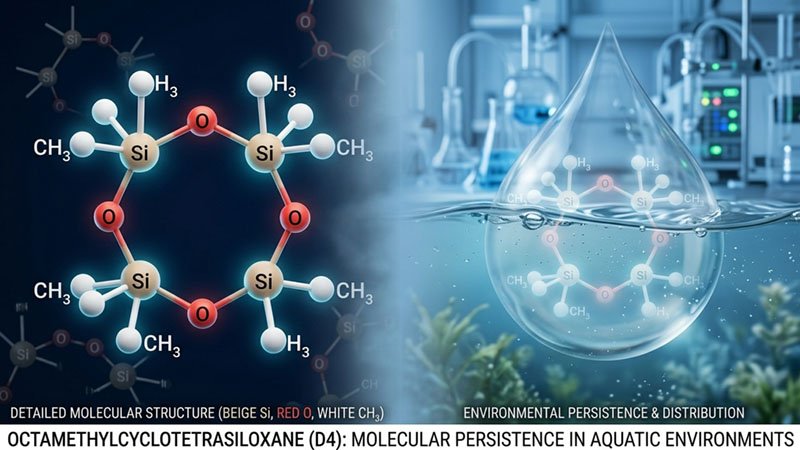
D4 (octamethylcyclotetrasiloxane), D5 (decamethylcyclopentasiloxane), and D6 (dodecamethylcyclohexasiloxane) are short cyclic siloxanes that are:
- Used as intermediates in making silicone polymer, not as ingredients in finished silicone parts.
- Listed as Substances of Very High Concern (SVHC) under EU REACH due to persistence and bioaccumulation in aquatic environments.
- Restricted to ≤ 0.1% w/w in wash-off cosmetic products in the EU (since 2020).
What this means for cured silicone parts:
- A finished, fully-cured, fully post-cured silicone bakeware or medical device contains trace residual D4/D5/D6 below 1,000 ppm in well-controlled compounds, and below detection in medical-grade material that has undergone 4-hour post-cure at 200 °C.
- Migration into food or skin is negligible under FDA and LFGB extraction conditions.
- Wash-off products (skincare, hair conditioners) using cyclomethicone fluids are a different conversation — that is liquid D5 used directly as an ingredient, not silicone polymer.
The regulatory concern is real, but it is upstream of the silicone supply chain. A platinum-cured silicone part with documented post-cure does not carry the same risk profile as a leave-on cyclomethicone cosmetic.
Skin Contact Safety
Silicone is one of the few polymers labeled hypoallergenic by default. It does not contain proteins, latex residues, or accelerators that drive Type I or Type IV skin sensitization.
- Type I (immediate) allergy is virtually unreported for cured silicone. Cases attributed to “silicone allergy” almost always trace to peroxide-cure residues, residual cleaning solvents, or unrelated pigments.
- Type IV (contact dermatitis) is rare; usually traces to a colorant, not the silicone itself.
- Skin barrier impact is low. Silicone does not strip lipids, alter pH, or block respiration. Wearables, scar sheets, and prosthetics rely on this.
See Is Silicone Hypoallergenic and Silicone Allergy for the deeper view, and Are Silicone Scrubbers Good for Your Skin for a cosmetics-side application.
Mouth, Body, and Medical Contact

Different contact types invoke different regulations. The cross-reference matters.
- Food contact: FDA 21 CFR 177.2600 + LFGB. Covers cooking, eating, drinking, food storage. For appliance specifics, see Is Silicone Safe in the Kitchen .
- Infant feeding: FDA + LFGB + (depending on jurisdiction) EN 14350 for drinking equipment, EN 1400 for soothers. See The Safety of Silicone in Baby Products.
- Mouth contact, non-food (vape mouthpieces, bong stems, straws): same FDA basis, but watch for hot-drink temperature limits and the distinction between stain and migration.
- Skin-contact medical devices: ISO 10993-5/10. See Biocompatibility Testing Pathways for Skin-Contact Devices.
- Short-term implants (≤ 30 days): USP Class VI minimum. Longer implant duration adds ISO 10993-6/11.
- Sterilization: silicone tolerates EO, gamma, and steam autoclave. The sterilization protocol affects long-term integrity — see Sterilization Methods and Their Impact on Medical Silicone.
For the structural answer to “can silicone go in the body,” see Is Silicone Truly Biocompatible for Medical Applications?.
Pigments, Fillers, and the “Fake Silicone” Problem
Most “silicone safety” failures are not silicone failures. They are:
- Non-FDA pigments. Silicone is colored at the masterbatch stage. Cheap suppliers reach for industrial pigments outside the FDA-approved colorant list. The polymer is safe; the dye is not.
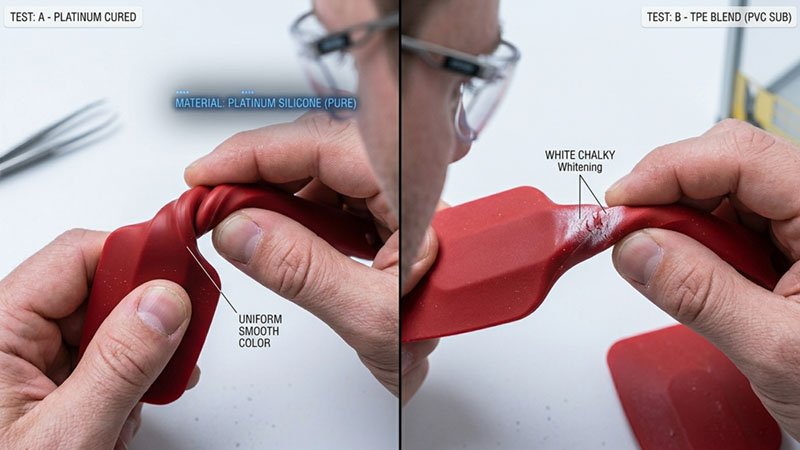
- Filler-loaded blends. Some “silicone” parts in the consumer market are TPR, PVC, or EVA blends with a small percentage of silicone fluid. They look and feel similar but carry plasticizer and heavy-metal risks. The pinch-and-twist test (whitening at the bend line indicates non-silicone filler) catches most of these.
- Peroxide cure without post-cure. Peroxide-cured silicone leaves residual byproducts — 2,4-dichlorobenzoic acid, benzoic acid, biphenyl — that are odor-active and outside FDA migration approval. Post-cure at 200 °C for 4 hours drives them off. See Silicone Products Post Cure and Platinum Vulcanization.
- Recycled or re-ground compound. Some bulk parts use a percentage of regrind. Acceptable for industrial use; not acceptable for food or medical without re-certification of the regrind batch.
If a part fails any of the above, the failure mode is the additive — not the silicone.
Environment and End-of-Life
Silicone is chemically stable, which is what makes it safe in use and inconvenient in disposal.
- Biodegradation is extremely slow under landfill conditions. Estimates range from 50 to 500 years. See How Long Does Silicone Take to Decompose.
- Hydrolysis eventually breaks silicone down to silica (SiO₂) and methane in soil — over geological timescales, not landfill timescales.
- Recycling is technically possible but not at scale. Most municipal programs do not accept silicone. Specialized recyclers exist for medical and industrial waste streams. See Can Silicone Be Recycled?.
- Microplastic shedding is minimal. Cured silicone does not fragment into microparticles the way polyethylene or PET do.
- Leachate is stable. Silicone in landfill does not release toxic leachate under normal pH and temperature.
The environmental conversation is real, but it is about persistence, not toxicity. Silicone is durable; durability becomes a disposal problem, not a contamination problem.
When Silicone Is NOT Safe
Five conditions remove the safety claim, even from a part labeled silicone:
- No compliance certificate, or certificate from a non-accredited lab. “Food grade” without a test report number and a lab accreditation is not a regulatory claim.
- Peroxide-cured without post-cure. Residue is outside FDA approval.
- Industrial-grade pigments or fillers. Common in low-cost consumer goods.
- Damaged surface. Cuts and burns expose untested filler-side material.
- Misuse beyond rated conditions. Bakeware over 230 °C, medical use of non-medical grade, or skin contact with industrial parts.
Quick Compliance Reference
| Use Case | Minimum Required Standard | Notes |
|---|---|---|
| Bakeware, food storage | FDA 21 CFR 177.2600 + LFGB §30/§31 | Platinum cure, food-approved pigments |
| Baby feeding, soothers | FDA + LFGB + EN 14350 / EN 1400 | Phthalate, BPA, and heavy-metal limits applied at part level |
| Skin contact, scar sheets | ISO 10993-5/10 | Cytotoxicity + skin sensitization + irritation |
| Short-term implant (≤ 30 d) | USP Class VI + ISO 10993-6 | Animal-model toxicity testing |
| Long-term implant (> 30 d) | ISO 10993-6/11/17 | Chronic toxicity, genotoxicity, biokinetics |
| EU consumer cosmetic | REACH (D4/D5/D6 ≤ 0.1%) | Applies to wash-off products containing cyclomethicone |
| California consumer goods | Prop 65 | Disclosure obligation if listed substances above safe-harbor |
FAQ
Is silicone carcinogenic?
No. Cured silicone polymer is not on the IARC or NTP carcinogen lists. The cyclic siloxane D4 is listed by ECHA as a substance of concern for aquatic toxicity and persistence — not as a human carcinogen.
Does silicone leach into food at high temperatures?
Properly food-grade, platinum-cured silicone tested under FDA 21 CFR 177.2600 conditions (water at reflux, 7 hours) shows extractables well below the 20 mg/in² limit. Peroxide-cured grades without post-cure can leach measurable byproducts.
Is silicone safe for babies and infants?
Yes — when the part carries both FDA and LFGB certification and uses platinum cure. Look for EN 14350 (drinking equipment) or EN 1400 (soothers) compliance on top of food-contact approval.
Is silicone a plastic?
No. Silicone is a synthetic rubber (elastomer) with an inorganic Si-O backbone. Most plastics use a carbon-carbon backbone. The distinction matters for both safety classification and recycling.
What This Article Does Not Cover
Three boundaries before generalizing any answer above:
- Silicone caulks and sealants are not the same product. Construction sealants release acetic acid or oxime during cure. They are not food-grade, not medical-grade, and not the subject of this article. Always reference the specific compound.
- Cyclomethicone in cosmetics is regulated separately. D4/D5/D6 used as liquid carriers in skincare are subject to REACH limits. The risk basis there is environmental persistence and bioaccumulation, not consumer toxicity at use levels.
- Compliance certificates apply by batch, not by brand. A supplier that was compliant two years ago is not automatically compliant on the shipment in front of you. Verify the report date, lot number, and accreditation on every order.
For deeper context on what silicone is and how it is made, see the Complete Silicone Material Guide. For the full property reference, see Properties of Silicone: Complete Material Guide.
Before signing off on any “safe silicone” claim, lock down four lines in writing:
- Polymer type (PDMS or specified grade)
- Cure system (platinum, with post-cure documentation if peroxide)
- Applicable certification (FDA / LFGB / USP / ISO 10993 by clause, with lab name and report date)
- Pigment and filler compliance (food-approved or medical-approved colorants only)
A safety claim missing any of those four lines is marketing, not regulatory documentation.








